PCO Puncher

Laparoscopic drilling of ovaries
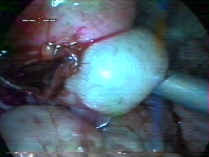
In women who fail to ovulate because of a condition called polycystic ovarian syndrome, if oral medications fail to achieve ovulation, laparoscopic drilling of the ovaries may be done. In polycystic ovaries, the ovaries are fully of tiny follicles with fluid in it. A few of these fluid filled follicles are punctured using an instrument introduced through the laparoscope. This causes reduced levels of hormones called androgens and subsequently there is restoration of normal ovulation. In the adjacent picture, the white organ is the ovary. the few brown spots seen on it are made by the electrocautery .
What to expect after this procedure:
Will my PCOD be totally cured?
In 82% of patients, ovulation can be expected. In 63% , conception can be expected either spontaneously or after treatment with medications to which they were previously resistant. It is cheaper compared to treatment with hormone injections. The effect may last longer. The rate of miscarriage in PCOD patients who concieve with laparoscopic drilling is slightly lower than that of women with PCOD who concieve with medical treatment. for those who respond to laparoscopic drilling, but relapse into anovulation, a repeat procedure has been shown to be effective . This procedure is particularly useful for slim women with PCOD.
Intrauterine Insemination

Intrauterine insemination involves the placement of motile sperms in the cavity of the uterus to enhance fertility.
Intrauterine insemination is indicated in couples when there is male infertility, or unexplained infertility, or in subfertility due to some other reason, where it is felt that intrauterine insemination will enhance fertility.
In normal fertile couples, semen is deposited in the vagina. Only a few sperms find their way in to the uterus in the normal course of events as many of them perish on their way up into the uterus traversing the sticky mucus in the mouth of the uterus, cervix, the opening of the uterus, etc. Intrauterine insemination increases the number of good motile sperms that reach the uterus, as good motile sperms are deposited directly inside the uterus.

In normal fertile couples, semen is deposited in the vagina. Only a few sperms find their way in to the uterus in the normal course of events as many of them perish on their way up into the uterus traversing the sticky mucus in the mouth of the uterus, cervix, the opening of the uterus, etc. Intrauterine insemination increases the number of good motile sperms that reach the uterus, as good motile sperms are deposited directly inside the uterus.
Ovulation Stimulation
Ovulation stimulation : In women with decreased ovulation or in women who need to undergo intrauterine insemination,
ovaries are stimulated with oral medications or injections to stimulate ovulation. The process is monitored with ultrasound monitoring of follicles starting on 10th day of menstruation.
Hysterolaparoscopy
Hysterolaparoscopy is a combination of laparoscopy and hysteroscopy usually done for infertile patients.It is usually done when tubal block is suspected, tubal cannulation or fimbrial block is expected, to correct endometriosis, or to remove ovarian adhesions.
Laparoscopy essentially means the visualization of the abdominal organs through a scope.Is.
A CCD camera is attached to the outer end of the laparoscope.
The uterus, ovary and the rest of the pelvic and abdominal organs can be visualized through the scope and viewed on a television monitor. Instruments passed through two tiny 5mm holes lower down in the abdomen can rectify any defects in the visualized organs . . It is usually combined with hysteroscopy.
Hysteroscopy visualizes the interior of the uterus and any polyps or adhesions can be removed.
Indications in the infertile woman: Laparoscopy as a primary modality for diagnosis of the infertile woman is no more practiced. Laparoscopy may be resorted to in the following situations
Laparoscopic drilling of ovaries
In women who fail to ovulate because of a condition called polycystic ovarian syndrome, if oral medications fail to achieve ovulation, laparoscopic drilling of the ovaries may be done. In polycystic ovaries, the ovaries are fully of tiny follicles with fluid in it. A few of these fluid filled follicles are punctured using an instrument introduced through the laparoscope. This causes reduced levels of hormones called androgens and subsequently there is restoration of normal ovulation. In the adjacent picture, the white organ is the ovary. the few brown spots seen on it are made by the electrocautery .
.jpg.crdownload)
What to expect after this procedure:
Will my PCOD be totally cured? In 82% of patients, ovulation can be expected. In 63% , conception can be expected either spontaneously or after treatment with medications to which they were previously resistant. It is cheaper compared to treatment with hormone injections. The effect may last longer. The rate of miscarriage in PCOD patients who concieve with laparoscopic drilling is slightly lower than that of women with PCOD who concieve with medical treatment. for those who respond to laparoscopic drilling, but relapse into anovulation, a repeat procedure has been shown to be effective . This procedure is particularly useful for slim women with PCOD.
Tubal block
If a woman fails to conceive inspite of medical treatment, it may be prudent to check and see if the fallopian tubes are patent. This can be achieved by injecting fluid into the uterus through a cannula introduced through the vagina. The fluid traverses the uterus , the fallopian tubes and then comes into the abdomen through the opening of the tubes called the fimbrial end. The fimbrial ends are visualized on the laparoscopy monitor . Any blocks near the fimbrial end or any adhesions near any part of the tube can be removed through laparoscopic instruments. If there is a block near the uterine end of the tube it can be rectified through hysteroscopic cannulation.
.jpg.crdownload)
Endometriosis
In some women, there may be severe abdominal cramps near the time of menstrual periods. This could be due to a disease called endometriosis. On examination of the vagina, the doctor may find some nodularities in the vagina. Endometriosis could cause infertility in many ways and the best way to correct it is through the laparoscope. Laparoscopic correction of endometriosis yields very high pregnancy rates. Adhesions between the uterus and ovaries could cause infertility and these could be corrected through the laparoscope. In the adjacent picture, there are adhesions between the ovary(The white organ) and the uterus (the pink organ) caused by endometriosis. The release of the adhesions with an instrument has resulted in some amount of bleeding , seen in the picture.
What it involves for the patient: The procedure is usually done under General anaesthesia. The patient’s basic blood investigations are done and she is given a laxative the previous night. Patients staying in the same district as the hospital are admitted on the same day of the surgery. The patient has to be nil by mouth on the day of the procedure.
After the procedure she is kept in the recovery room for about 3-4 hours and then taken to her room. Usually the patient is discharged on the next day in our centre.